
++++++++++++++++++
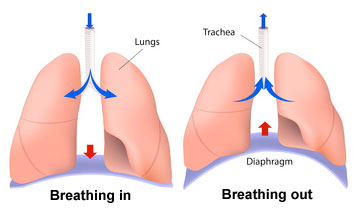
On exhalation, the diaphragm and intercostal muscles relax and return to their resting positions. This reduces the size of the thoracic cavity, thereby increasing the pressure and forcing air out of the lungs.
++++++++++++++Air is moved through the lungs by a ventilating mechanism, consisting of the thoracic cage, intercostal muscles, diaphragm, and elastic components of the lung tissue.